The Four Layers of Continuity
A framework for extending care beyond appointments.
The first two articles in this series named two structural problems most care organizations share.
The 167-Hour Problem: established that most care systems only touch a small fraction of a person's week, and that the most consequential moments often happen in the hours no system currently owns.
The Documentation Trap: established that recording care is not the same as sustaining it.
Both point toward the same conclusion: continuity does not happen automatically. It must be intentionally designed. So the question becomes practical: what does intentional continuity actually look like?
After examining how organizations across behavioral health, higher education, victim services, and social services attempt to bridge the gap between appointments, a consistent pattern emerges.
Continuity is not a single intervention. It is not a feature. It is a layered system, and every layer serves a distinct function no other layer can replace.
We call this framework
The Four Layers of Continuity.
Layer 1
Layer 2
Layer 3
Layer 4
Sessions. Appointments. Case reviews. Support groups.
These are the formal touch points of care: the layer most organizations already design for, fund for, and measure. Without scheduled care, there is no structure.
Scheduled Care
But it is only a foundation. An appointment creates a moment of support.
Continuity determines what happens after the appointment ends. Organizations operating exclusively within Layer 1 find that progress built during sessions often struggles to survive the days between them.
If a client stops attending, how long before your organization notices? If the answer is measured in weeks, Layer 1 is likely where continuity ends.
Layer 2 extends care beyond the formal encounter: structured check-ins, follow-up communication, and proactive outreach that does not require a crisis to activate.
Most organizations attempt some version of this. The challenge is consistency.
Support here typically depends on individual staff effort rather than organizational design. As caseloads grow, Layer 2 is the first to erode. Not because anyone decided it wasn't important, but because no system is holding it in place.
Support should not disappear when appointments end.
Between-Session Support

Can your organization describe, in concrete terms, how clients are supported between appointments, or does that depend primarily on individual staff initiative?
Many organizations assume continuity requires constant staff involvement. It does not.
Layer 3 makes support available when providers are not: educational resources, guided exercises, self-directed tools, crisis planning materials.
Resource Accessibility
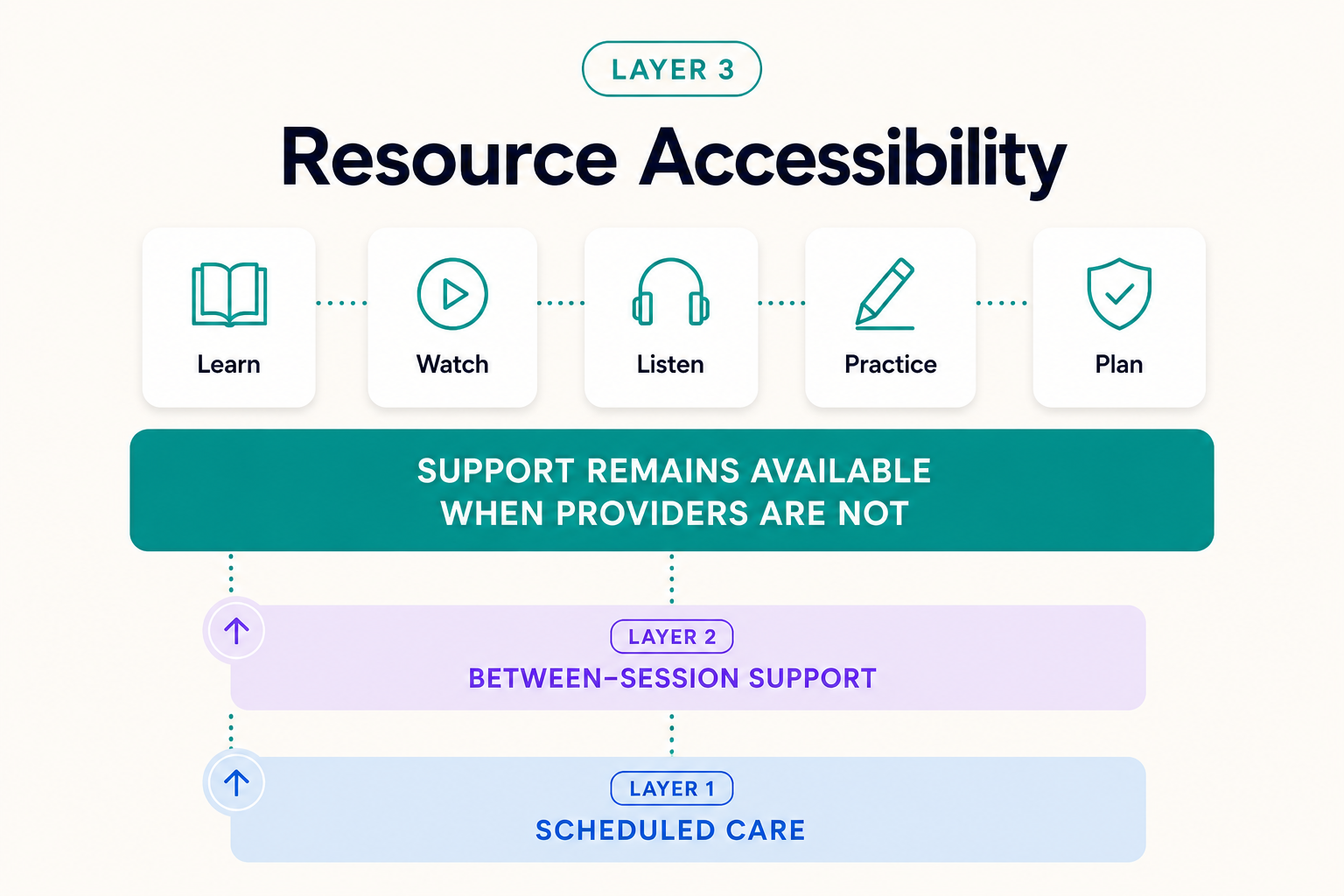
The purpose is not to replace providers. It is to ensure the space between appointments is not simply empty.
The question shifts from Can we be available at all times? to Can support remain available even when we are not? Only the second is solvable at scale.
When clients encounter difficulty between appointments, what structured support is available that does not require a staff member to initiate it?
Continuity Visibility
This is the layer most organizations are missing, and the one that transforms continuity from a delivery function into an organizational capability.
Layer 4 creates structured awareness of how clients are doing between appointments: engagement patterns, early signs of disengagement, changes in wellbeing over time.
Without it, organizations discover challenges after they have already become crises. Leaders have strong documentation of what happened in sessions and almost no insight into what is happening between them.
Organizations cannot support what they cannot see.
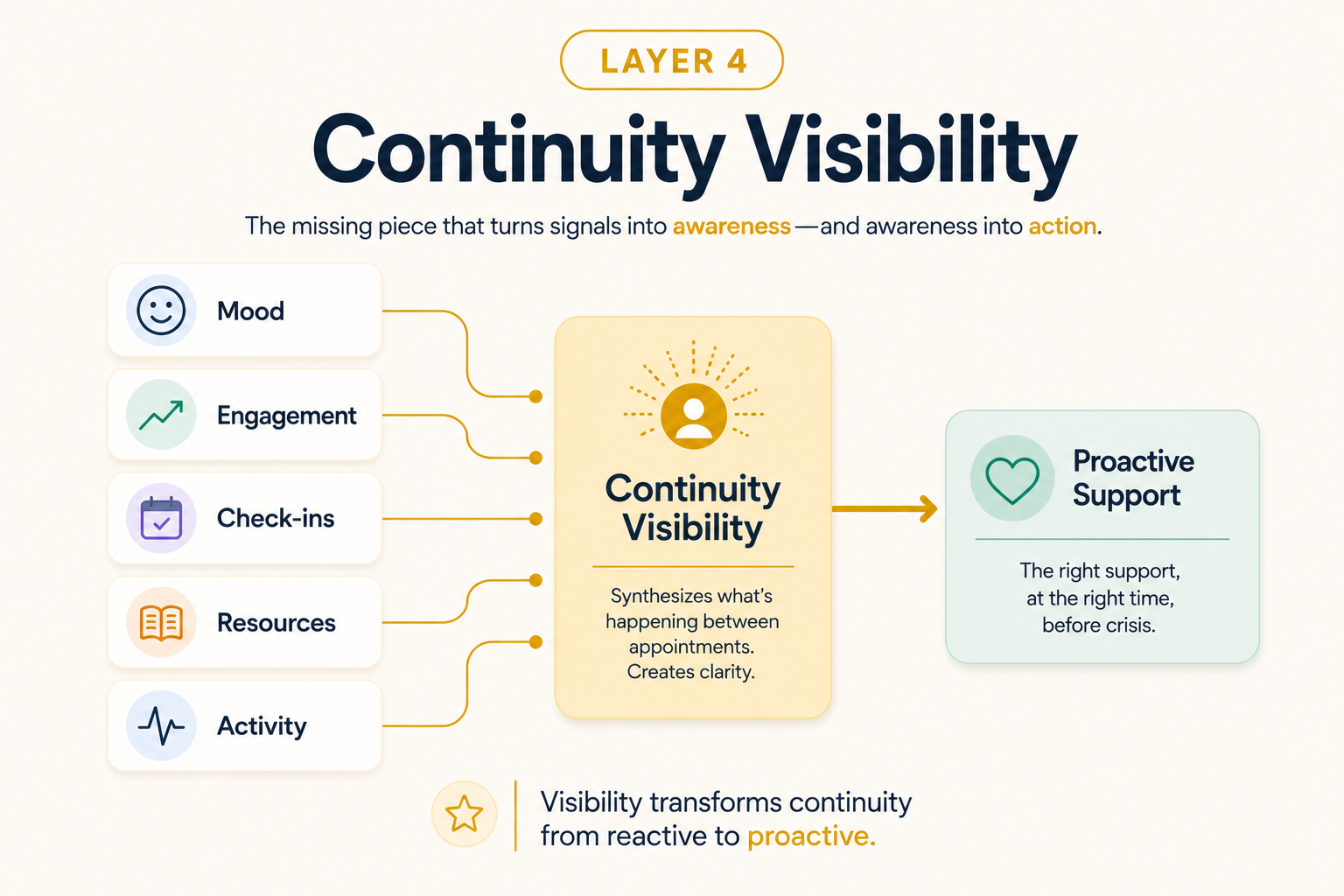
Layer 4 is not surveillance. It is the awareness that allows care to be proactive rather than reactive.
Does your organization have any structured mechanism for understanding how clients are doing between appointments — as patterns emerge, not after the fact?
Why Most Organizations Stop at Layer 1
The answer is rarely a lack of commitment. It is a lack of infrastructure. Most care systems were designed around appointments. Most funding models support encounters, not engagement between them.
Most documentation systems capture what happened, not what is happening.
As a result, organizations wanting to deliver more than Layer 1 have historically built continuity through extraordinary individual effort. That effort is admirable. It is not a system.
"Effort does not scale. Infrastructure does."
The Layers Work Together
The layers are cumulative, not interchangeable. Each contributes something no other layer can provide.

Where Does Your Organization Sit?
Most leaders can describe their scheduled care model fluently. Fewer can describe how they support clients between appointments. Fewer still can explain how their organization maintains visibility into client wellbeing between sessions.
That gap is not a failure of leadership. It is a predictable consequence of building care systems around appointments rather than continuity.
The question is not whether your organization cares about continuity. The question is which layers are currently in place, and which, if strengthened, would most change outcomes for the people you serve.
"Continuity is not built all at once. It is built layer by layer."
Natural next step
Understanding the framework is the beginning. Knowing where your organization sits within it is what makes it actionable.
The Continuity Audit is a structured self-assessment that helps Executive Directors, Program Directors, and Case Management Leaders identify which layers are operational, and where the highest-leverage opportunities lie.