The Documentation Trap
We Confused Documentation With Continuity of Care. Most Organizations Still Do.
Most organizations have invested significantly in documentation infrastructure.
Documentation and continuity serve different functions. Confusing them is one of the most consequential design errors in human services — and most organizations don't know they've made it.
Most organizations have invested significantly in documentation infrastructure. Case notes. Session summaries. Client records. Compliance systems. Outcome reporting tools.
These investments are legitimate and necessary. Regulatory compliance, institutional accountability, and clinical standards all depend on rigorous documentation. No serious argument exists against it.
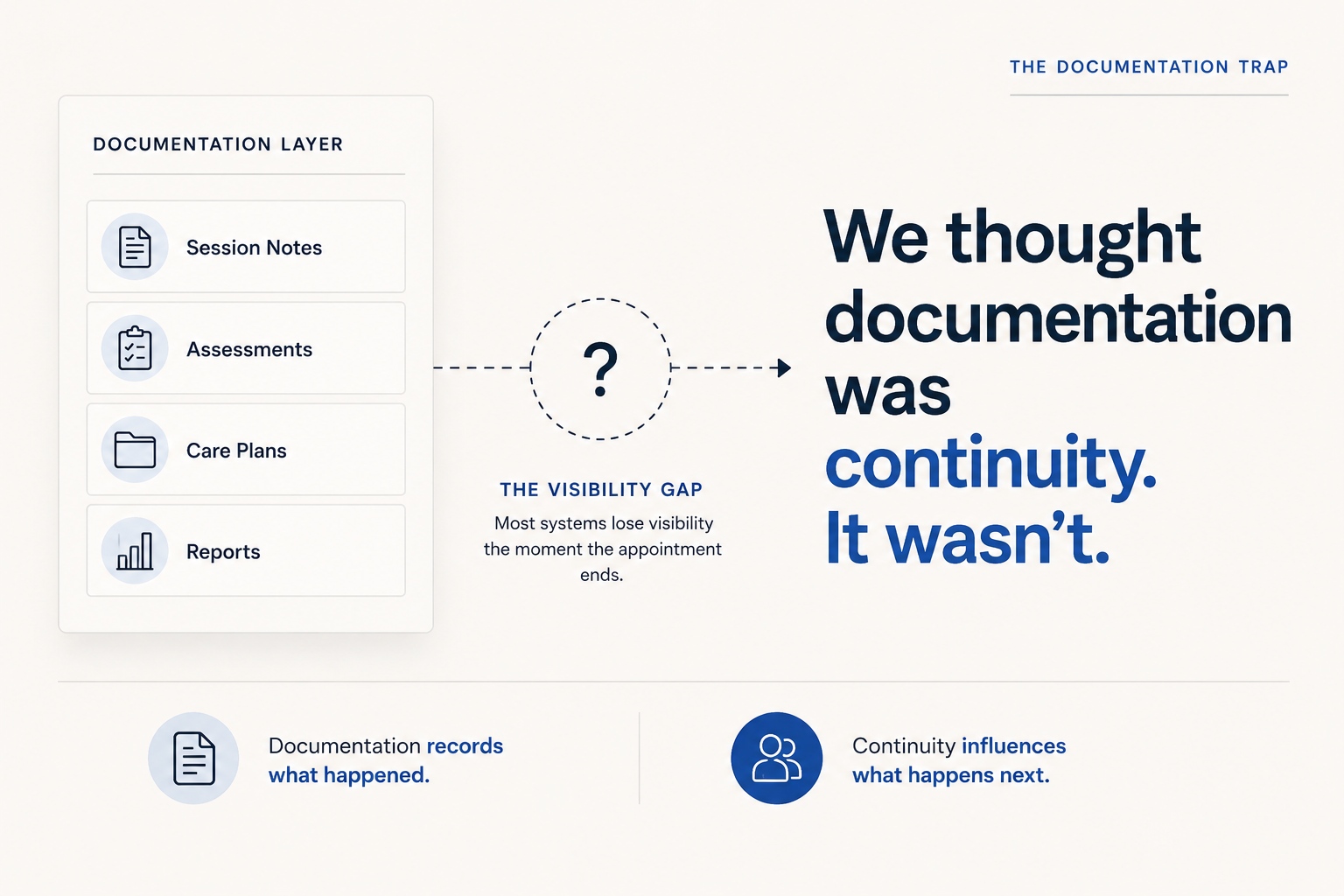
But somewhere along the way, documentation became a proxy for something it was never designed to provide: continuity of care.
The Documentation Trap
The assumption that because care has been recorded, continuity has been achieved.
It is one of the most common, and most consequential, misconceptions in human services, behavioral health, and case management today.
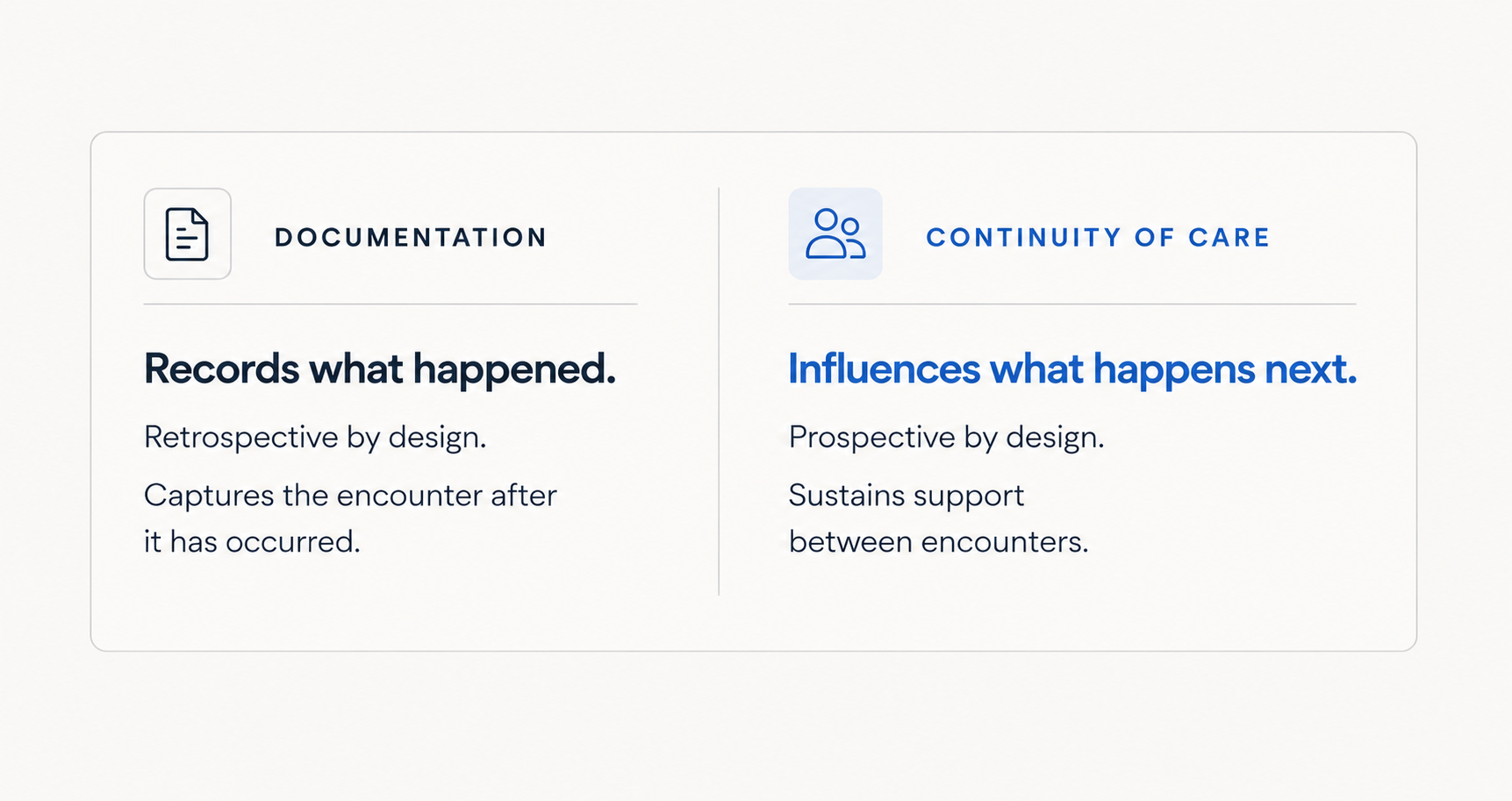
Documentation and continuity of care are not the same function
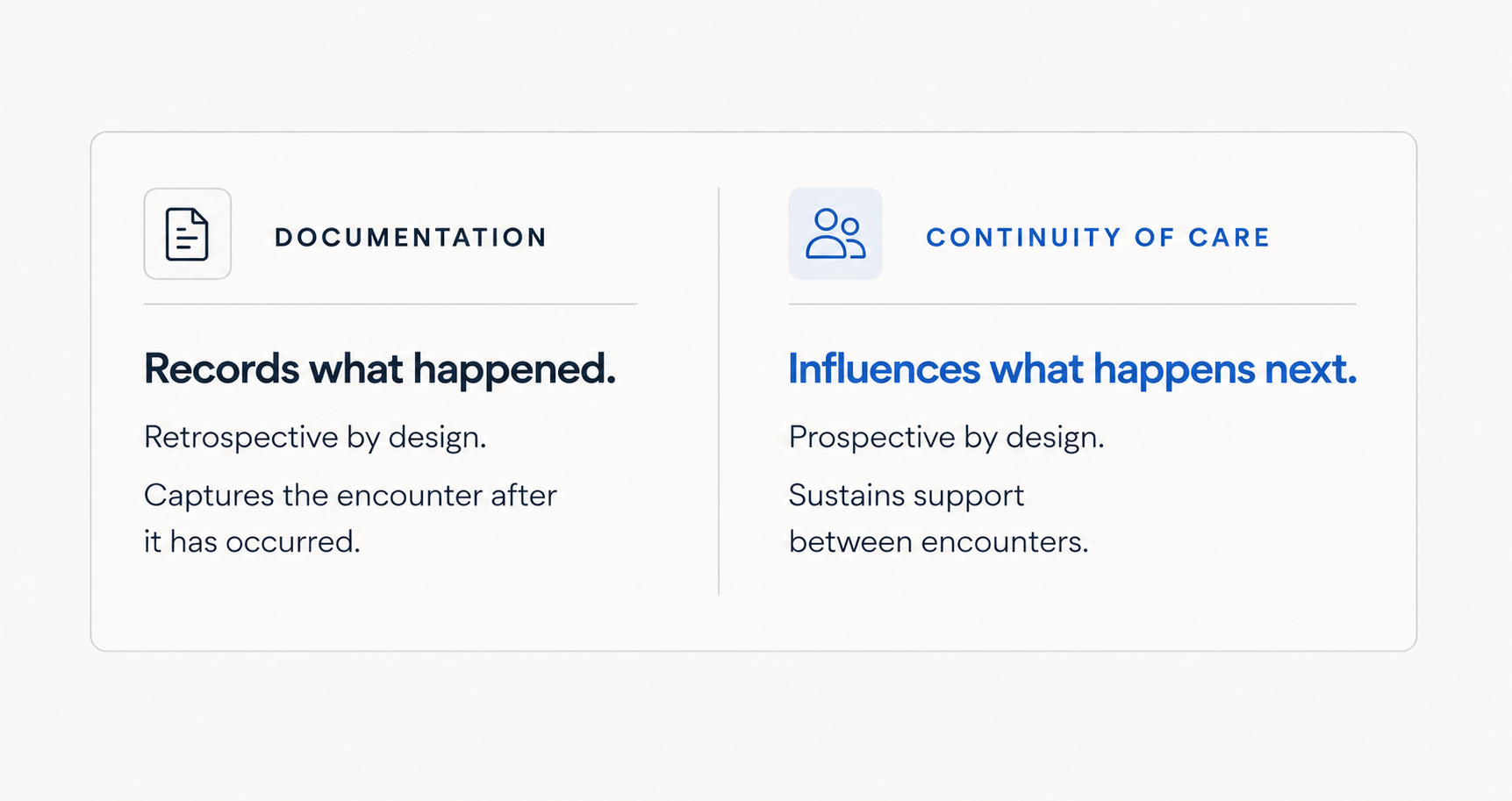
- Documentation preserves information. Continuity preserves momentum.
- Documentation captures the encounter. Continuity supports the journey.
- Documentation closes a record.
Continuity keeps the connection open.
Both are necessary. But they serve fundamentally different operational purposes — and confusing one for the other creates a blind spot at the center of most care delivery models.
The practical consequence is this: a provider may have complete and accurate documentation of every session and still have almost no visibility into what is happening between them.
They may not know how a client is managing three days after a difficult session — whether engagement is quietly declining, whether recommended resources were accessed, or whether new stressors have emerged that will surface as a crisis at the next appointment.
"A provider can have a complete record of every session and still have almost no visibility into what is actually happening."
Documentation tells them what happened. It offers no mechanism for understanding what is happening now.
→ Related: The 167-Hour Problem
The operational gap this creates, and why it compounds
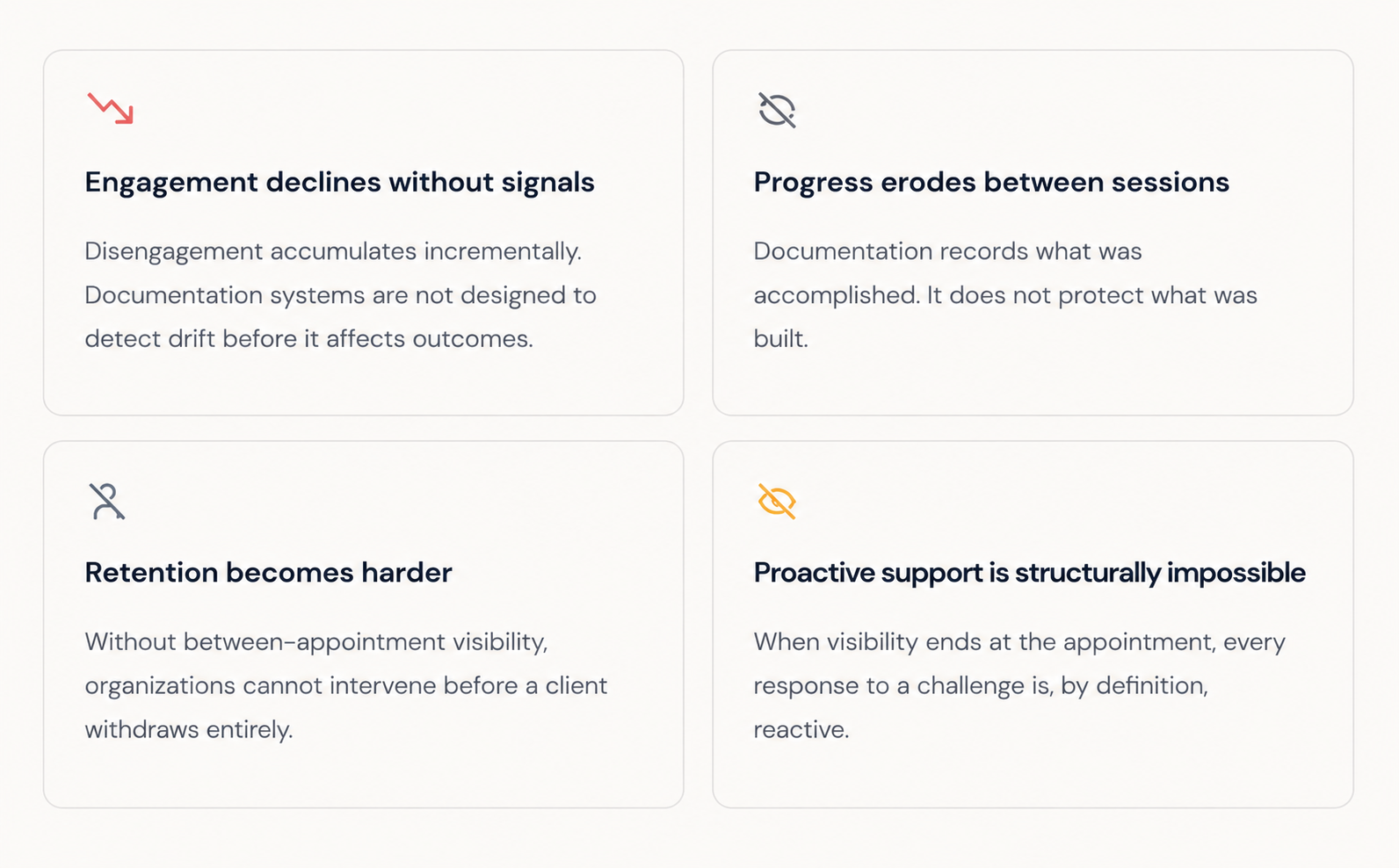
Organizations that fall into the Documentation Trap tend to share a recognizable pattern: they operate reactively. Critical information arrives after the fact. Providers discover challenges at the next scheduled session rather than when they first emerge.
Early intervention windows — the moments when a timely connection might have meaningfully changed a client's trajectory — pass undetected.
This is not a staffing problem. It is not a training problem. It is a continuity design problem. The system was built to capture care. It was not built to sustain it.
Why this distinction matters for organizational outcomes
For Executive Directors, Program Directors, and Case Management Leaders, the Documentation Trap is not a philosophical concern. It has direct consequences for the outcomes organizations are accountable for delivering.
The organizations beginning to close this gap are not adding more appointments or more staff. They are redesigning how support is delivered between touchpoints, creating systems that sustain engagement, preserve progress, and provide care coordination across the full arc of the client experience.
"Documentation records care. Continuity extends care."
Continuity of care requires its own operational layer
A genuine continuity framework does not replace documentation — it extends beyond it. It creates the conditions for engagement, visibility, and care coordination to exist between appointments, not only within them.
Organizations building toward continuity are asking different operational questions:
This shift reflects a deeper change in operational philosophy — from care as a series of documented encounters to care as an ongoing relationship between touchpoints.
Continuity is not a feature that can be added to an existing documentation system. It is a distinct operational discipline, and it requires its own design.
The question worth asking in your own organization
If your organization were to examine what it currently knows about client experience between appointments (not from records, but from active engagement) what would the answer reveal?
For most organizations, that question exposes the true shape of the gap. The Documentation Trap is not a failure of intention. It is a failure of design. And design problems require design solutions.
What continuity of care looks like in practice
If continuity requires more than documentation (and the evidence suggests it does) the natural next question is structural:
What does a continuity framework actually consist of? What are its components? And how do organizations begin building toward it?
Most leaders, when they first encounter this distinction, find the concept immediately recognizable but the operational path forward less obvious.
Understanding that documentation and continuity serve different functions is the first step. Understanding how to structure, layer, and sustain continuity across a diverse caseload is the second.
Continue reading
The Four Layers of Continuity offers a practical framework for understanding how organizations can extend support beyond the appointment and begin closing the gap between what documentation records and what clients actually experience between sessions.